To the Editor:
Bowling Green City Council is considering mandatory mask-wearing in stores, shops, and other public buildings, and in crowded outdoor areas where safe physical distance cannot be maintained, to protect everyone from the SARS-CoV-2 (“Corona”) virus which causes the COVID-19 pandemic. Because COVID-19 is being spread by people who don’t have symptoms, and therefore don’t know they have it, and because not enough testing is available for us to know who is infected, we are forced to play “Russian roulette” with COVID-19. Face masks and physical distancing are the only “bullet vests” available to protect ourselves and those we care about in this game. The virus can cause serious illness in people of any age, including children, and there is no way to predict whether you will have a mild or severe illness.
By wearing masks in stores and businesses, we protect the people who risk their lives to serve us, as well as other customers. We also protect our healthcare workers from physical exhaustion and the unbearable task of making difficult ethical choices of life and death, which will result if our hospitals are overrun with too many infected people, as is now happening in many other states.
Below, I present the relevant scientific information in question-answer format about the SARS-CoV-2 (“Corona”) virus, and the COVID-19 pandemic it causes. My goal is to explain why we must take this action now to protect the people of Bowling Green from the dangerous spread of the virus.
Wearing masks is a small sacrifice we should all make to protect each other.
Neocles Leontis
Professor of Chemistry, BGSU
Bowling Green City Council, at-large representative
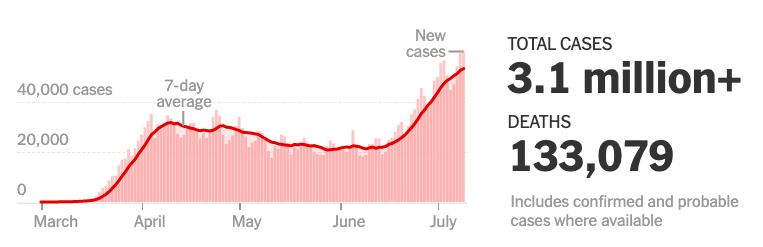
- How many have been infected by SARS-CoV-2 or died? As of July 10, 3.1 million Americans have been infected (25% of the world’s 12.2 million cases) and 133,000 Americans have died (25% of the world’s 555,000 deaths). The US has only 4.2% of the world’s population, yet one quarter of all the cases and deaths worldwide. By contrast, China, where the virus originated, has 1.4 billion people (18.% of the world’s population) but only 90,400 cases and 4,641 deaths (less than 1% of world cases and deaths). While new cases have been reduced to near zero in China, they are dangerously increasing in the US, including Ohio and Wood County. (See Ref 1)
New cases in United States are increasing:
New cases in Ohio are increasing:

By contrast, Germany has brought the pandemic under control:

- Is there a cure? There is still no known cure and no available vaccine for COVID-19. Currently, the pandemic can only be stopped by effective preventive measures, including face masks. Note that, so far, we have been unable to create effective vaccines against any other corona viruses that infect humans or animals. Clinical trials of the anti-malarial drug hydroxychloroquine show that it provides no benefit for COVID-19 patients. Recently, two widely used antiviral drugs used for HIV (lopinavir and ritonavir) also failed to cure COVID-19. Ref 2
- Who is susceptible to infection? Because this is a new virus, everyone is susceptible to infection, unless (a) you already survived the infection and (b) you have immunity. Even if you survive, you may not have immunity in the future. Because we are a long way from “herd immunity,” which, for this virus, requires that at least 70% of Americans (200 million people) get infected, your chances of getting infected keep increasing as the disease spreads. Ref 3
- How is the virus spread? The virus spreads in microscopic droplets (aerosol effect) that we emit into the air when we speak and breathe normally. These minute droplets can remain suspended in the air for many minutes and then be inhaled by others, causing new infections. The evidence is outlined in a letter by 200 scientists to the World Health Organization. Ref 4
- Why does the virus spread so rapidly? First, because it is airborne and second because it can be spread by people who don’t have symptoms or feel sick, and don’t even know they are infected! The virus is treacherous and insidious. Without testing everyone, we don’t know who is infected and who isn’t. (Ref 5)
- How many infected people do not have symptoms? About 40% to 45% of people with SARS-CoV-2 infections do not have symptoms, but they can transmit the virus to others for an extended period, perhaps longer than 14 days. Because of the high risk for silent spread, testing programs must include people without symptoms if we are going to stop the pandemic. Ref 5
- How many infections are spread by people without symptoms? A large percentage of infections will continue to be spread by people without symptoms. Ref 6
- How do we stop the spread? The most effective way to stop the spread of this virus is to test everyone to identify contagious people and isolate and treat them. Since we do not have adequate testing in the US, we don’t know who has the virus, especially those that show few or no symptoms. Therefore, we must rely on the second most effective way: Everyone must wear masks in public spaces, especially indoors, maintain at least 6 feet physical distance from others, and frequently wash their hands. Note that distance alone is not enough because the microscopic droplets have been shown to travel long distances, even across a large room, before falling to the floor. Staying six feet away from an infected person may not protect you, unless you both wear masks. (Ref 7)
- Are masks effective? Mandated face coverings, such as those implemented in China, Italy, and New York City, effectively prevented airborne transmission by blocking atomization and inhalation of virus-bearing microscopic droplets. Simultaneous use of face covering, social distancing, together with extensive testing and contact-tracing, was credited for the curve flattening in China and is the most optimal approach. Ref 8
- How long does immunity last? We do not know whether people develop immunity to this virus or, if they do, how long immunity lasts after recovery from the disease. Studies of other coronaviruses suggest immunity might only last a few months. Therefore, we should assume that reinfection by SARS-CoV-2 is possible for those who survive a first infection. Ref 9
- Is the virus changing? Like other RNA viruses, the SARS-CoV-2 virus mutates rapidly. Already a new variant has emerged (D614G) having a change in the spike protein that binds to ACE-2 receptors on human cells. Just in the last few months, the mutated virus has spread rapidly worldwide, replacing the original, because it appears to be more infectious or easier to replicate. Ref 10
- Does the virus only affect our lungs? In addition to respiratory symptoms due to lung infection, the virus also infects heart, liver, kidneys, intestines, brain, and, in fact, any organ that has the ACE-2 receptor protein on its cell membranes. Serious side effects include blood clotting in blood vessels that can lead to strokes, heart attacks, and even gangrene, possibly requiring amputations. Ref 11
- Does it only affect seniors? No. Serious and even deadly infections of people in their teens, 20s, 30s or 40s also occur. Recently 41-year old actor Nick Cordero died of COVID-19, due to severe clotting which required doctors to amputate his legs. This was not enough to save him. “A young person who has no real medical co-morbidities, but gets super sick and ends up on multiple support machines is a clinical portrait that doctors are now seeing a lot,” said Dr. Taison Bell, a physician specializing in infectious diseases, and pulmonary and critical care at the University of Virginia. Ref 12
- Who is most at risk of severe COVID-19 illness or death? According to the CDC, your risk of being hospitalized, entering the ICU, being put on a ventilator or dying increases with age. In addition, you are at greater risk if your BMI (body mass index) is 30 or greater or if you have type 2 diabetes. Ref 13 For example, your BMI is 30 if you are 5 foot 6 inches tall and weigh 185 pounds. You can calculate your BMI at this link.
- How long does it take to recover from COVID-19? Recovery can take a long time and permanent damage to organs can occur. A recent study found that 87.4% of patients who were discharged from the hospital after recovery from COVID had persistent symptoms, especially fatigue and difficulty breathing and 44% reported decreased quality of life Ref 14
- In which states is COVID-19 increasing and where is it decreasing? Unfortunately, the United States does not have a national policy for dealing with COVID-19, so states have been left on their own to decide what to do. Ref 15 The virus is now spreading rapidly in precisely those states that closed too late and opened their economics too soon, and where social distancing and wearing of face-masks was not enforced: Texas, Florida, South Carolina, Mississippi, and Arizona, among others. On the other hand, the virus is under control in those states that closed early, opened slowly, require face masks in public, and have effective contact-tracing (e.g. New York, New Jersey, Massachusetts, Connecticut, Rhode Island, etc.). Ohio opened without full protective measures and now is in danger of imminent spread. Ref 16
- How have other countries succeeded in stopping the spread of the virus? Many other countries have brought the virus under control through effective national policies that include widespread and frequent testing, mandatory mask wearing, physical distancing, and effective contact tracing. Countries such as South Korea have done so without shutting down their economies, as we were forced to do because we did not act soon enough to prevent the pandemic. Ref 17
- What is contact-tracing? To stop the pandemic we must identify everyone who has come into contact with any person known to be infected. This is contact-tracing. Then those people need to be safely isolated and treated until they are well. Countries that have stopped the epidemic house quarantined individuals in special hotels, where they provide food, medical care, and pay their salaries so they can take care of their families. Ref 18
- Will we need more lock-downs? If everyone wears masks in public places, and if we implement effective contact-tracing, we can avoid future lock-downs and economic disruptions. If we do not, more lock-downs will be inevitable.
- What is the Infection Fatality Rate (IFR)? This is the number of people who die divided by the actual number of infections. Since we don’t know exactly how many are infected in any region, this number has to be estimated. The consensus at a recent meeting of 1,300 scientists is that the IFR in the US is about 0.6%, which means that the risk of death in the country is less than 1%. This percentage may seem very small, but 0.6% means 47 million people in the world and 2 million Americans will die – so the virus remains a major threat. This situation can worsen, and the IFR can increase, when infected people overwhelm our hospitals and there are not enough health workers and ICU beds for them. Ref 19
- How many people have actually been infected already? According to CDC data, there are probably 10 additional cases for every documented infection.This means that instead of 3.1 million, closer to 31 million people have already been infected in the US. Most of these people don’t have symptoms but can still spread the disease. Ref 20
- What are Case Fatality Rates (CFR)? This is the number of people who die from COVID-19 divided by the number of known cases. China has a CFR of 5.1 % (4,641 deaths/90,400). The United States has a similar CFR of 4.3% (133,000 deaths/3.1 million cases). But case fatality rates vary wildly: Iceland’s is less than 1%, New Zealand’s and Israel’s are below 2%. Belgium, by comparison, is at 16%, and Italy and Britain at 14%. When hospitals are overwhelmed and healthcare workers can’t cope with all the infections, more fatalities occur. In addition, routine treatments for heart attacks and cancer are disrupted, leading to more deaths. Ref 21
- Are 99% of COVID-19 cases really “totally harmless”? The death rate does not capture all of the harm caused by the disease. According to some estimates, 15%-20% of known COVID-19 patients require hospitalization, and of these, 15%-20% are transferred into intensive care. Roughly 1 in 20 (5%) become critically ill. Many will suffer debilitating long-term effects, including impaired lung function, neurological problems and cognitive deficits, and some may require lifelong care and not regain full independence. Ref 14
- What are the short-term effects of COVID-19? At first, you may develop a fever, dry cough, sore throat, or head and body aches. You may lose your sense of smell. Your fevers and weakness may last for weeks on end. You may have internal clotting leading to strokes, seizures, confusion, and brain inflammation or heart attacks, cardiac inflammation, and impaired circulation to arms and feet. You may develop acute respiratory distress syndrome (ARDS) if your alveoli – the tiny air sacs of their lungs – become infected and stuffed with fluid, white blood cells, mucus, and the remains of destroyed lung cells. This causes your blood oxygen levels to plummet and you struggle ever harder to breathe. In this case you are likely to end up on a ventilator and may die.
- What are the long-term effects of COVID-19? Residual symptoms such as continuing shortness of breath, muscle weakness, flashbacks and mental fogginess can persist for some time. Many patients suffer debilitating long-term effects, including impaired lung function, neurological problems and cognitive deficits, and some may require lifelong care and not regain full independence. Ref 23
- How does COVID-19 kill you? The virus acts like no pathogen humanity has ever seen. It can infect many organs, including the heart and blood vessels, kidneys, gut, and brain. Patients can die from respiratory failure (ARDS), heart or kidney failure, blood clots, or an overzealous immune response (“cytokine storm”). Ref 23
- How can we quickly monitor overall viral load in our community? We can do this by measuring the amount of virus in municipal waste every week. Ref 24
- What do we still have to learn about this virus? There are still many things to learn. We do not know (1) why there is so much variation in the severity of the disease in different people, particularly between young and older individuals as well as men and women; (2) the nature of the immunity humans develop against this virus or how long this immunity lasts; (3) which mutations of this virus are potentially dangerous; (4) how well vaccines will work to prevent new infections; (5) the exact origin of the virus, in particular, whether it passed directly to humans from horseshoe bats or through intermediate species of animals; (6) how it causes such widespread damage to the human body; (7) to what degree infected children can transmit the virus. Ref 25
References:
- Coronavirus Map: Tracking the Global Outbreak and Worldometer website and Johns Hopkins Coronavirus Global Map and COVID-19 Act Now
- Which drugs and therapies are proven to work, and which ones don’t, for COVID-19?
A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe COVID-19
Three big studies dim hopes that hydroxychloroquine can treat or prevent COVID-19
- Mayo Clinic: Herd immunity and COVID-19 (coronavirus): What you need to know
- Identifying airborne transmission as the dominant route for the spread of COVID-19
239 Experts With One Big Claim: The Coronavirus Is Airborne
Letter from 239 Scientists: It is Time to Address Airborne Transmission of COVID-19
Airborne Coronavirus: What You Should Do Now How to protect yourself from a virus that may be floating indoors? - Prevalence of Asymptomatic SARS-CoV-2 Infection
Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control COVID-19 - Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2)
- Masks for Prevention of Respiratory Virus Infections, Including SARS-CoV-2, in Health Care and Community Settings: A Living Rapid Review
How Face Masks Can Help Prevent the Spread of COVID-19 - These Two Studies Show How China Flattened The Coronavirus Curve
The effect of human mobility and control measures on the COVID-19 epidemic in China - Scientists report rapid loss of COVID-19 antibodies
The time course of the immune response to experimental coronavirus infection of man - This coronavirus mutation has taken over the world. Scientists are trying to understand why.
- How COVID-19 can damage the brain
Central Nervous System Involvement by Severe Acute Respiratory Syndrome coronavirus-2 (SARS-CoV-2)
Platelet Gene Expression and Function in COVID-19 Patients - 41-year actor Nick Cordero dies of COVID-19
Coronavirus Infections in Children Including COVID-19 An Overview of the Epidemiology, Clinical Features, Diagnosis, Treatment and Prevention Options in Children
Mayo Clinic: COVID-19 (coronavirus) in babies and children - OpenSAFELY: factors associated with COVID-19 death in 17 million patients
CDC updates, expands list of people at risk of severe COVID-19 illness
Why COVID-19 kills some people and spares others. Here’s what scientists are finding.
Here’s What Recovery From COVID-19 Looks Like for Many Survivors: Continuing shortness of breath, muscle weakness, flashbacks, mental fogginess plague patients for a long time.
Persistent Symptoms in Patients After Acute COVID-19
Months into the pandemic, many U.S. cities still lack testing capacity
State-level tracking of COVID-19 in the United States
How South Korea Flattened the Curve The country showed that it is possible to contain the coronavirus without shutting down the economy
- What is contact tracing?
- The Pandemic’s Big Mystery: How Deadly Is the Coronavirus?
- Seroprevalence of Antibodies to SARS-CoV-2 in Six Sites in the United States, March 23-May 3, 2020
- Heart conditions drove spike in deaths beyond those attributed to COVID-19, analysis shows
- Genes May Leave Some People More Vulnerable to Severe COVID-19
DNA Inherited From Neanderthals May Increase Risk of COVID-19
Analysis of ACE2 Genetic Variability among Populations Highlights a Possible Link with COVID-19-Related Neurological Complications - How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes
How corona virus enters cells – lecture 2020 - SARS-CoV-2 RNA concentrations in primary municipal sewage sludge as a leading indicator of COVID-19 outbreak dynamics
A New Generation of Fast Coronavirus Tests Is Coming: But it will likely be months before these tests hit clinics. - Six months of coronavirus: the mysteries scientists are still racing to solve
Up to half of hospitalized patients have enzyme levels that signal a struggling liver
Kidney damage is common in severe cases and makes death more likely. The virus may attack the kidneys directly, or kidney failure may be part of whole-body events like plummeting blood pressure.
Intestines
Patient reports and biopsy data suggest the virus can infect the lower gastrointestinal tract, which is rich in ACE2 receptors. Some 20% or more of patients have diarrhea.
The need for dialysis may be because the kidneys, abundantly endowed with ACE2 receptors, present another viral target.
How does the virus enter cells? When an infected person expels virus-laden droplets and someone else inhales them, the novel coronavirus, called SARS-CoV-2, enters the nose and throat. It finds a welcome home in the lining of the nose, according to a preprint from scientists at the Wellcome Sanger Institute and elsewhere. They found that cells there are rich in a cell-surface receptor called angiotensin-converting enzyme 2 (ACE2). Throughout the body, the presence of ACE2, which normally helps regulate blood pressure, marks tissues vulnerable to infection, because the virus requires that receptor to enter a cell. Once inside, the virus hijacks the cell’s machinery, making myriad copies of itself and invading new cells.
What is a cytokine storm? The driving force in many gravely ill patients’ downhill trajectories is a disastrous overreaction of the immune system known as a “cytokine storm,” which other viral infections are known to trigger. Cytokines are chemical signaling molecules that guide a healthy immune response; but in a cytokine storm, levels of certain cytokines soar far beyond what’s needed, and immune cells start to attack healthy tissues. Blood vessels leak, blood pressure drops, clots form, and catastrophic organ failure can ensue.